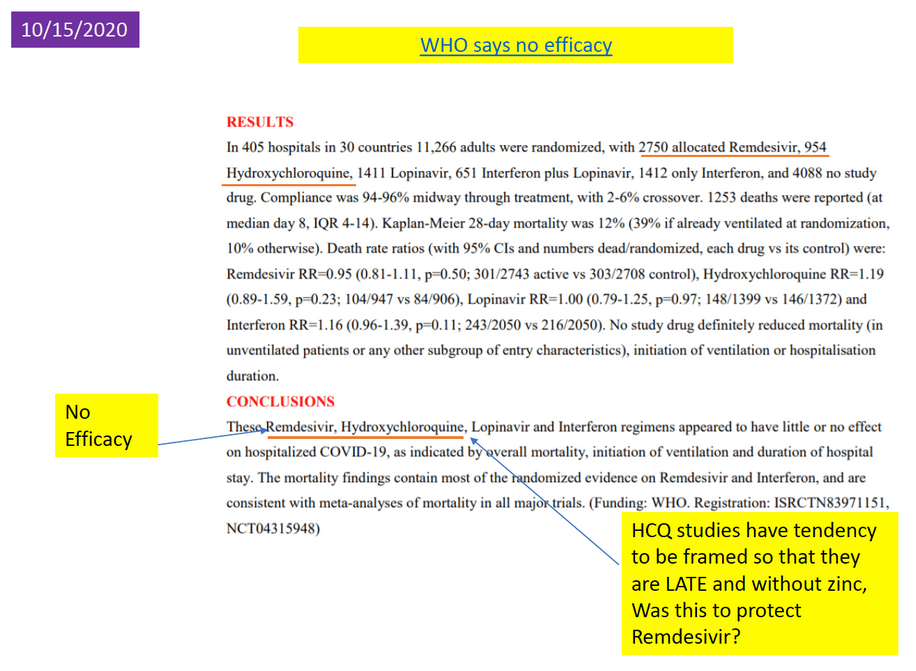
“WHO has issued a conditional recommendation against the use of remdesivir in hospitalized patients, regardless of disease severity, as there is currently no evidence that remdesivir improves survival and other outcomes in these patients.” World Health Organization.
Remdesivir is a highly toxic drug that medical officials advocate in the fight against Covid. But what is it, and why do the same officials ferociously defend it when there are known side effects that are deadly? The FDA approved it under the name Veklury for IVs in non-hospitalized outpatient treatment on January 27, 2022. They also terminated approval of two monoclonal antibody drugs, saying they “didn’t work” for the Omicron variant. Those two drugs had known life-extending properties for Covid patients. Let’s have a look at the controversy and why there may be more to this than meets the eye.
Failed Drug
Remdesivir was developed in 2009 by Gilead Sciences to treat hepatitis C and respiratory syncytial virus (RSV), but it didn’t work against those diseases. So they “repurposed” it for Ebola and Marburg viruses in 2014. It wasn’t effective in stopping the replication of those viruses either. Now it has once again been “repurposed” for Covid. But the narrative of the NIH is that it does stop the replication of the SARS-Cov-2 virus. It is not recommended for treating Covid patients, but that hasn’t stopped the ‘powers that be.’
RAIR Foundation USA spoke to an infectious diseases physician for this article involved in early clinical trials for Remdesivir at the beginning of the pandemic. She told us that Remdesivir was not effective for patients severely afflicted with Covid. They actually stopped the trials when they saw that patients’ kidney and/or liver functions were elevating. In medical terminology, this is called: increased alanine transaminase or aspartate transaminase – these are the enzymes secreted by the liver or kidneys that can shut down during an IV of Remdesivir.
So why in the world would the FDA approve a drug that must be monitored for kidney/liver failure? The FDA now approves the drug to treat “non-hospitalized patients.” The drug is administered through an IV, and patients must be closely monitored. But non-hospitalized?
Doctors have sounded the alarm for months, but their voices have fallen on deaf ears.
In this strange situation, we have the FDA revoking approval of the known life-extending drugs containing monoclonal antibodies, Regeneron being one of the two that were revoked. They say the drugs do nothing for the Omicron variant, which they claim is 99% of current cases. Omicron is the least dangerous of the variants. Take an aspirin and a cup of hot lemon tea and skip it. The only monoclonal antibody drug they left for use is Sotrovimab. Our doctor told us that there are two therapeutics she has used that work: Dexamethasone (a steroid that reduces inflammation) and monoclonal antibodies like Sotrovimab. But why revoke the antibody drugs and leave the known bad drug?
Dr. Death – the Fauci connection
Remember the problem of overuse of antibiotics? Use them too long, and the bacteria find a way to mutate around them. The same principle applies to antiviral medicines, which is one reason variants continue to emerge. Remdesivir is also a failed drug – even during Ebola studies, it was found to do little for patients afflicted with the virus and was actually highly toxic.
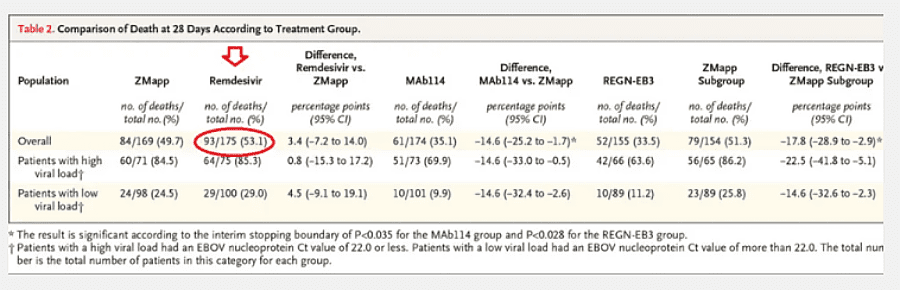
Monoclonal antibodies, which mimic the body’s creation of antibodies against disease, were more effective then, as they are now. ”Remdesivir had a 53% death rate which is considerably higher than that of Covid”.
As opposed to the lowest death rate of the monoclonal antibody drug Regeneron. With Covid, Remdesivir statistics from 2,058 deaths on CMS data (Medicare) revealed a death rate of 26%, and 46% of those died within 14 days of treatment. The mortality rate from Covid is around 1%, depending on the country.
Dr. Anthony Fauci advocated for Remdesivir therapy in April of 2020. In his own citation of the Gilead study, 53 people from the US, Canada, Europe, and Japan, reported 60% adverse events – from renal failure to liver problems to multiple organ failure. The NIH even now warns about renal failure and liver toxicity from Remdesivir. The World Health Organization (WHO) – does not recommend it for use in Covid patients. Fauci does.
WHO has issued a conditional recommendation against the use of remdesivir in hospitalized patients, regardless of disease severity, as there is currently no evidence that remdesivir improves survival and other outcomes in these patients.” World Health Organization
So we have a so-called “expert” doctor who advocates for a treatment that is known to kill and is not effective against the Covid virus. We have a Federal Agency that is also advocating it be used for Covid patients knowing full well that it can kill. That same agency pulled the life-saving monoclonal antibody treatments known to save lives. In the face of all the information against Remdesivir, it appears the Federal government and its experts are not “listening to the science” at all.
Creating more deaths for the PANDEMIC Narrative
According to the CDC, the average age of someone dying from COVID-19 is 82 years. The average life span of an American is 80 years. data.cdc.gov/NCHS/Provisional-COVID-19-Death-Counts-by-Sex-Age-and-S/9bhg-hcku



Recent Comments